Understanding Survival Statistics | What They Mean – and What They Don’t Mean
By PCRI
Survival. It’s a huge word. Yet science uses it often, and without pause. It is a statistic. But for the cancer patient, the word survival is more than a statistic. It is one of the most personal statements about him and his cancer journey. It deserves more than common reference, and more understanding of its true definition. For the newly diagnosed prostate cancer patient, survival is one of the first thoughts. But we are still learning how to explain more clearly that every prostate cancer is different, and the majority do not even shorten survival.
For the man with recurrent prostate cancer, the issue of survival resurfaces. Once again, he is wondering if someone can really tell him how long he’ll “survive” with this cancer. Often he is shocked by his own recurrence – perhaps he was told he was “cured”.
For the castrate-resistant (or hormone-refractory) patient, concerns about mortality are even greater. Preoccupation with survival is heightened by media reports of high drug prices coupled with “months” of extended survival. This has accompanied virtually every newly approved prostate cancer drug since 2010, including PROVENGE, Zytiga, Xtandi, and now Xofigo. This tends to leave a man trying to do his own personal math – measuring his survival in definitive months or years, based on the small amount of information he has received on “median overall survival”. This article will help show you how that type of calculating almost always underestimates survival.
Newly Diagnosed & "Survival"
For the newly diagnosed man, survival is often his first thought, and can instill fear for a long time. This fear often leads to a rushed treatment decision, even though it is recommended that a man take time to make his treatment choice. One of the steps in the treatment process is to understand what risk category his cancer fits into. (See August 2012, PCRI Insights - Newly Diagnosed: Understanding your Risk) Is he High Risk? Intermediate Risk? Low Risk? Or Very Low Risk? The Risk Category calculations most widely used are probably these three: 1.) D'Amico 2.) NCCN 3.) CAPRA Score. Of these three, only CAPRA Score measures survival – Progression Free Survival to be exact (at 10 years). But it is important to remember that many things can change in the 10 years after diagnosis, especially new drug approvals. And even the CAPRA is changing with time and newly available tests. Ongoing clinical trials are currently integrating a prostatectomy pathology testing called Decipher. This test is showing the ability to "down-risk" some men who originally had a High Risk Capra Score. (1)
D'Amico and NCCN Guidelines only measure risk of PSA recurrence after surgery or radiation (at 5 years), not survival. So a newly diagnosed man who is in D’Amico or NCCN’s High Risk category is at high risk of PSA recurrence after surgery or radiation – not at high risk of dying. Although we can argue that the recurrence rates and survival rates are related, they are not synonymous. Many men who have recurrence die from other causes, not prostate cancer. Therefore, it is important that a man understand what he’s being told he’s at risk for.
It is also important to remember that nothing in science is perfect, including statistics. In fact, to illustrate this with statistics themselves – nothing is 100% accurate, including survival statistics. They are meant to be probabilities and calculated estimates based on certain (but not all) variables. One of the leaders in statistical analysis, the National Cancer Institute, states it this way – “Because survival statistics are based on large groups of people, they cannot be used to predict exactly what will happen to an individual patient...doctors cannot be absolutely certain about the outcome for an individual patient.” (2)
Prostate Cancer Recurrence & Survival
Whether a man has PSA-only recurrence (aka biochemical recurrence) or metastatic recurrence after treatment, the issue of survival resurfaces. He is again faced with the question – “How long can I live?”
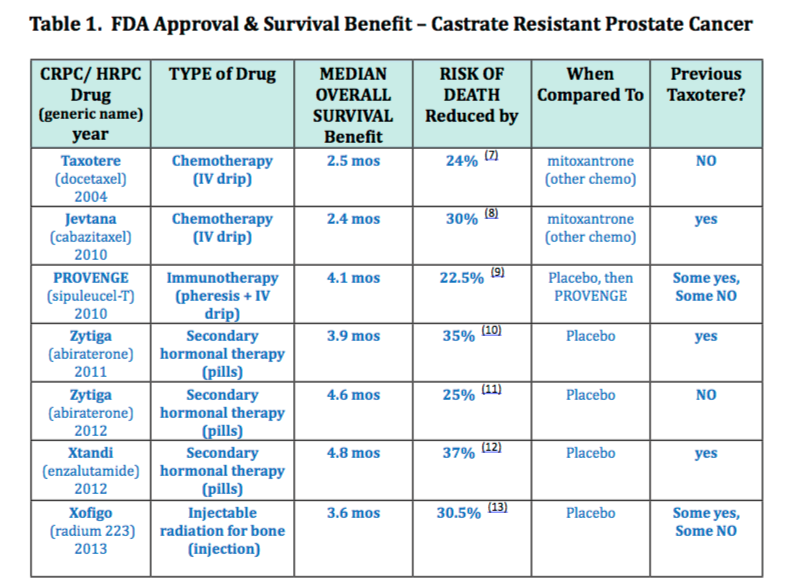
Once again, there are no exact measurements of survival with recurrence, only statistics. Studies can give estimates, but Dr. Marc Garnick from Harvard reminds us, "Remember that average survival times are based on studies of men treated in the past, and sometimes as long as 10 or 20 years ago." (3) So, they cannot factor in new treatments available after those 20 years. Table 1 (see below) represents the pace of new drug approvals over recent years-treatments which significantly prolong a man's survival. Dr. Garnick goes on to say that some of the studies that measured survival “...included men who did not undergo further treatment after biochemical recurrence occurred. It’s likely that these men would have survived for a longer time if they had received additional treatment after biochemical recurrence was detected...For these reasons, the “average” chances may be much better for a man treated today.”
...average survival times are based on studies of men treated in the past, and sometimes as long as 10 or 20 years ago.” Marc Garnick, MD Harvard Health Publications
CRPC- Median Overall Survival & the FDA
The FDA considers survival measurement to be the “most reliable cancer endpoint for measuring treatment effectiveness.” (4) In the 70’s, the FDA approved cancer drugs by assessing tumor response, called Objective Response Rate (ORR). However, from the 80’s on, the focus became survival data because it was considered “...more direct evidence of clinical benefit...” and superior to ORR. Because of this, pharmaceutical companies design their clinical trials around survival measurements- Overall Survival (OS) to be exact.
Overall Survival is defined by the FDA as this - "the time from randomization until the time of death from any cause..." (5) The term "randomization" refers to the process in a clinical trail, where people are randomly assigned to different groups, or different "arms". (6)
Median is not the average. It is actually the true middle number. In statistics, the average is called “mean”. Most of us understand the concept of average (mean) better than middle number (median), but statistics regards median as a more pure number. It is less influenced by isolated values that are extremely high or extremely low, which are called “outliers”. As a patient, perhaps I would want to know those numbers, both the highs and the lows. However a statistician would argue that they only skew pure statistical results.

Figure 1. Median is not the average. It is the true middle number.
So Median Overall Survival (MOS) is a statistic where the middle number is pulled out of a large collection of data which has measured death from any cause (not just cancer). MOS is what the FDA requires from a clinical trial for a cancer drug to receive its FDA approval.
Since 2010, we have seen several drugs receive FDA approval for men with castrate resistant prostate cancer. Each time a drug is approved, the Median Overall Survival benefit is quoted (see Table 1). This leaves men and their families thinking this is a finite number that applies to them personally and often trying to weigh out the months of promised life against the expensive price tag associated with the new drug. Since these are the two numbers that inevitably make the news, this type of “math” is not surprising. However, let me shed more light on more numbers which should help give a broader perspective and change up the mathematics a little.
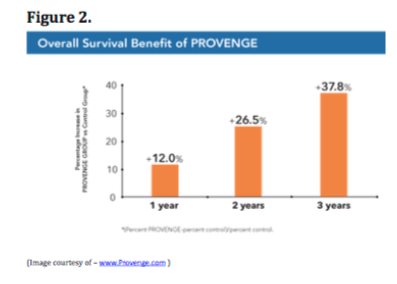
When a drug is FDA approved, the pharmaceutical companies are highly regulated in what they can print and say. For example, they are not allowed to make claims about their drug that weren’t in the published Product Information (PI) document approved by the FDA. The PI document may quote the Median Overall Survival, but usually doesn’t mention the mean (average) or the range in overall survival from the studies. So MOS is often the only number we’re given, although some companies have found an alternative FDA approved way to report their data. In Figure 2, Dendreon, the manufacturer of Provenge, illustrates the percentage likelihood of increased survival three years in the future compared to men who were treated with placebo.
Things We Cannot Measure
As Dr. Garnick pointed out previously, studies cannot measure everything. They cannot measure the impact of new treatments that will come to market years after the statistics were published. They cannot measure the advocacy of a wife or family member and the impact it has on choosing better treatments. They cannot measure the positive choices a cancer patient makes in his journey, such as dietary and lifestyle changes, preventing side effects, or speaking up at a doctor’s appointment.
As the National Cancer Institute pointed out, nothing in science is perfect, including statistics. They are probabilities and excellent percentages. However, that is still different than perfection. The power of future change and the choices a cancer patient makes cannot be measured. Yet they are very real.
Fear of Death
This is a difficult subject to discuss but since I was forced to face it head-on for 13 years with my husband, it is something I’m ready to talk about. Dominic lost his cancer battle in April 2013 – 13 years and 1 month after his diagnosis of widely metastatic prostate cancer. This type of journey brings out every emotion you can name, and magnifies them at times. Some of them are familiar – some of them are a surprise. But the one emotion I had to face most over those 13 years was simply fear. Fear of losing my husband – fear of my son losing his father – and every other fear that goes with it. Sometimes I would retreat to deal with the feelings. Often I would pray. But, I was a busy caretaker, so long car rides to do errands often became my getaway. I did find this one simple truth; facing my fears made me a better advocate for my family. But I had to retreat to do it. Running away from my fears only made me more anxious and fearful. I believe that facing your fears is an important element of patient empowerment and especially advocacy. It makes you stronger, not weaker. Find some time to do this for yourself and the ones you love.
Define the Odds
The prostate cancer community is full of men who have beaten the odds, defying the survival statistics they were quoted by their physicians. I will continue to argue that getting involved in your cancer care, or “patient empowerment”, is one of the most significant factors. This is based on what I have seen in 11 years on Helpline and 13 years of advocating for my husband who was diagnosed with a PSA of 7,096. He had extensive bone mets for all those years – and again, lived for 13.
We beat all odds and every statistic you could throw at us. I knew his medical records, listened to his needs and desires, and was greatly responsible for ordering tests and choosing treatments. This was because we had a wonderful oncologist who listened to us and knew how our situation was different, including my job and my involvement in advocacy. His expertise guided us, but ultimately Dominic was in the lead. We often changed decisions on a weekly basis simply because that’s what Dominic needed or wanted. We listened to him, and we listened to his medical records – key to patient empowerment.
Here are more stories from men who have castrate resistant prostate cancer and have beaten the odds. Most of them also have metastatic disease. These men are part of a longstanding Email Support Group, which you can find on www.HRPCA.org.
Personal Stories – Beating the Odds
• Donald & Nancy - “Yes indeed, I was “given” 3-5 years - more than 10 years ago and I’m still rolling along fine.”
• Dan J. - “I was given a year, five and half years ago,”
• Jan Burgess - “Gord was given 6 months – 13.5 years ago!!!”
• Joyce O. - “My husband isn’t here to testify, but he lived 15 years after his diagnosis. He was told he had 2-3 years to live by a radiation oncologist...He didn’t die of prostate cancer 15 years later, but of a heart attack. I felt he lasted so long because of our research of all the effective treatments that were available.....Keep on fighting!“
• Kirby B. - “I was given 16-24 months on diagnosis Feb. 7, 2000. PSA was 87 with spread to pelvic lymph nodes. I am now 13 years out and still golfing.”
• Don Q. - “I am pleased to report that I have now achieved my 15th year since diagnosis of PCa ...Doc told my wife 18 months. ...Survival largely due to doing research and finding the right Docs, treatments and medicines, natural and otherwise. Fortunately still fairly fit and enjoy life. Regards”
• Ron A. - “At diagnosis Gleason 9s and a PSA of 12.8, I was told that my Ca was advanced and aggressive and that the only option was hormonal palliative care. That without it I would be dead in two years..It will be 7 years in November since I was diagnosed ...If I could advise any of you of one thing it is to watch your weight, diet, and exercise. We more often die of heart disease before the cancer gets us.”
• Michael J. - “I was diagnosed with Stage IV metastatic PCa on December 23, 1999, and given less than 9 months to live....Dr. Myers has fought two reoccurrences with me and I am working part time and living a very active life. I am writing from the French Countryside where I played golf yesterday. Never give up!”
Let this article be a reminder that survival statistics are never perfect and were never intended to be. Let it also be a reminder that people truly beat the odds every day, and becoming involved in your treatment decisions is one of the most powerful factors in beating any odds or statistics that you were given.
Originally published in PCRI Insights, August 2013, Vol. 16: No. 3